

On November 1, 2023, the Centers for Medicare & Medicaid Services (CMS) released the Calendar Year (CY) 2024 Home Health Prospective Payment System Rate Update and Home Infusion Therapy Services Payment Update Final Rule. The rule, effective on January 1, 2024, contains final policies related to the Medicare home health benefit for CY 2024 on payment and quality-related programs.
Key Takeaways from the 2024 HH Final Rule
The CY 2024 Final Rule includes some mitigation of the proposed -5.65 percent downward permanent behavioral adjustment to the 30-day payment rate resulting in an estimated +0.8 percent overall impact for home health providers in CY 2024. However, CMS still applied a reduction of -2.89 percent that eliminates much of the benefit of the annual payment update and continues a policy that is anticipated to result in further, potentially significant payment reductions in future years. While these payment updates are certainly preferred to the CY 2024 Proposed Rule, they still create challenges for providers that have dealt with significant inflation, staffing issues, and other cost increases.
The CMS final rule for Home Health 2024 includes a number of key takeaways that we will break down in this post, including:
- Base rate increase: The base rate for home health services will increase by $27.44, from $2,010.69 to $2,038.13.
- Behavioral adjustment: The home health prospective payment system (HH PPS) base rate will be impacted by a –2.89% permanent adjustment as part of CMS’ ongoing analysis of behavioral changes under PDGM. The overall impact of this permanent adjustment will be a 2.6% reduction in spending, as the adjustment is not applied to LUPAs.
-
- The Final Rule also details the potential for a future temporary adjustment to account for what CMS views as $3,489,523,364 in overspending from 2020 through 2022.
- Other factors in setting the CY2024 base rate include a 3.0% payment update based on the market basket and a 0.4% increase resulting from the updated fixed-dollar loss (FDL) ratio used to manage outlier payments.
HHQRP Changes
Home Health Quality Reporting Program (HHQRP)
- The CMS is adopting two new measures beginning with CY 2025
-
- Discharge Function Score (DC Function)
- COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date
- The CMS is removing one existing measure and two OASIS-E items
-
- Application of Percent of Long-Term Care Hospital (LTCH) Patients with an Admission and Discharge Functional Assessment and a Care Plan That Addresses Function
- M0110 – Episode Timing
- M2220 – Therapy Needs
- This rule finalized a requirement for public reporting of four measures in the HH QRP
-
- The below measures will be reported in the January 2025 Care Compare refresh
-
-
- DC Function measure
- Transfer of Health (TOH) Information to the Provider—Post-Acute Care (PAC) Measure (TOH-Provider)
- Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) Measure (TOH-Patient)
-
-
- The below measure will be reported in the January 2026 Care Compare refresh
-
-
- COVID-19 Vaccine: Percent of Patients/Residents Who Are Up to Date
-
- Codified the 90 percent data submission threshold policy in the Code of Federal Regulations
HHVBP Changes - Value-Based Purchasing
Expanded Home Health Value-Based Purchasing (HHVBP)
Beginning in CY 2025 the below measures will be removed:
- OASIS-based Discharged to Community
- Both Total Normalized Composite measures
- Acute Care Hospitalization in the first 60 days
- ED Use without Hospitalization in the first 60 days
Beginning in CY 2025 the below measures will be added:
- Claims-based Discharge to Community-Post Acute Care (DTC-PAC)
- OASIS-based Discharge Function Score (DC Function)
- Claims-based Home Health Within-Stay Potentially Preventable Hospitalization (PPH)
Due to the removal and addition of measures the weights of each measure will be updated as per the table below: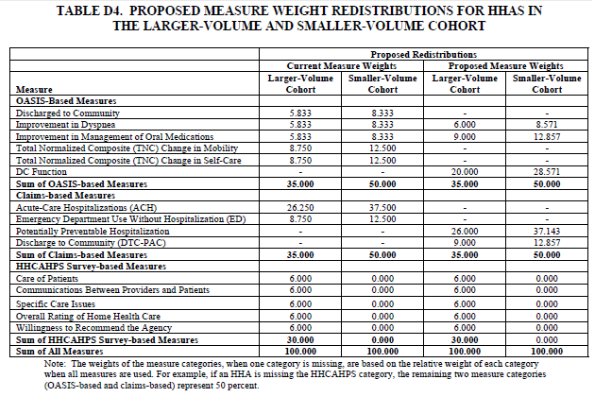
- Update the Model baseline year from CY 2022 to CY 2023 starting in the CY 2025 performance year
Home health agencies should review the final rule to understand all changes being implemented. The CMS is also providing resources to help home health agencies implement the changes.
Data Takeaways
- Wage Index
-
- 33 rural CBSAs have reduction - 4 rural max 5% reduction (AZ, MA, HI, WA, NH), 15 rural CBSAs have an increase – 1 over 5% (ND at +10.92%)
- 244 urban CBSAs have reduction - 41 max 5% reduction, 166 urban CBSAs have an increase – 22 over 5%
- LUPAs
-
- 16 HHRGs have 1 fewer visit needed to reach the threshold, 25 have 1 more visit, and 391 remain the same
Case Mix Weight Recalibration
-
- 258 HHRGs lower CMW than 2023, 173 HHRGs higher, 1 same
- By Clinical Grouping, see list below:
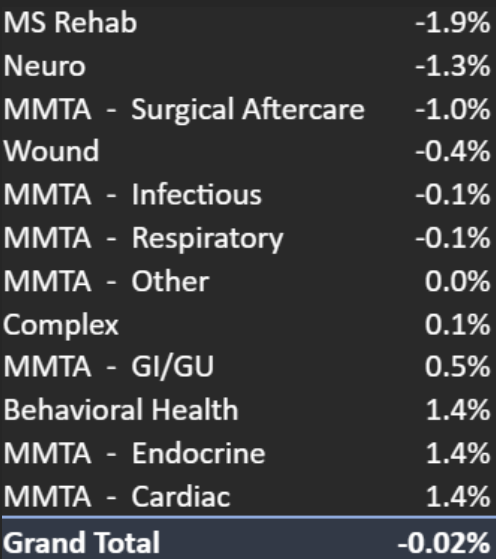
Home Health Aide Utilization
In the 2024 Proposed Rule, CMS requested comments and feedback regarding an identified decrease in home health aide utilization over the past few years. The Final Rule summarizes common causes received from commenters, along with an indication that CMS will be continuing to review this perceived issue. The key pieces of feedback called out in the rule are listed below.
While this is not specifically stated in the rule, it is possible that CMS will include some of these items in future audits.
- Beliefs that CMS has not been effective at cracking down on agencies that do not appropriately utilize aids, especially with higher acuity patients.
- Perception that the PDGM model discourages agencies from providing aides leading to miscommunication to patients.
- Recruitment and retention issues for labor competition in other markets, low compensation, inadequate training, and demanding work conditions.
- Reimbursement does not support robust staffing in rural areas where nurses or occupational therapists can provide the same service.
- Differences in coordination with Medicaid state by state.
- Physicians hesitant to include on care plans due to agency feedback of staffing being limited or not available.
- Agencies are hesitant to utilize aides if families/caregivers are not willing to learn to perform these tasks independently.
Hospice Impacts
Special Focus Program:
The 2024 HHA Final Rule finalizes the algorithm to identify the poor-performing hospice programs using Hospice surveys, Hospice Care Index Overall Score, and four CAHPS Hospice Survey measures. Hospice programs identified as the ten percent with the highest scores, which represent the lowest-performing hospices, will be considered for participation in the Special Focus Program.
Hospice Informal Dispute Resolution (IDR) for hospice programs would allow hospice providers an informal opportunity to refute one or more condition-level deficiencies cited in the Statement of Deficiencies survey report, which would align with the established IDR for Home Health Agencies.
The 36-month rule for hospice providers was finalized aligning the regulation with the existing Home Health regulation. The final rule forbids any change in majority leadership during the 36 months (about 3 years) after an initial Medicare enrollment, including acquisitions, stock transitions or mergers.
2024 Physician Final Rule
CMS is finalizing its proposal to modify the requirements for the hospice Conditions of Participation (CoPs) to allow social workers, MHCs, or MFTs to serve as members of the interdisciplinary group (IDG) and removing the proposed language requiring that the determination regarding whether a social worker, MFT or MHC serve as a member of the IDG depending on the preferences and needs of the patient.
The 2024 Physician Fee Schedule Final Rule was also published this week with impacts for Palliative Care, Home Health, Outpatient Therapy, and Behavioral Health.
CMS is finalizing a regulatory change to allow for the general supervision of therapy assistants by PTPPs and OTPPs for remote therapeutic monitoring (RTM) services.
Finalizes a payment for Caregiver Training when practitioners train caregivers to support patients with certain diseases or illnesses (e.g., dementia) in carrying out a treatment plan. Medicare will pay for these services when furnished by a physician or a non-physician practitioner (nurse practitioners, clinical nurse specialists, certified nurse-midwives, physician assistants, and clinical psychologists) or therapist (physical therapist, occupational therapist, or speech-language pathologist) as part of the patient’s individualized treatment plan or therapy plan of care.
The 2024 final rule includes a separate payment for Community Health Integration, Social Determinants of Health (SDOH) Risk Assessment, and Principal Illness Navigation services to account for resources when clinicians involve certain types of health care support staff such as community health workers, care navigators, and peer support specialists in furnishing medically necessary care. This will also include new codes for these services.
There will be a new add-on code G2211 to recognize resource costs for evaluation and management visits for primary care and longitudinal care, recognizing the inherent costs involved when clinicians are the continuing focal point for all needed services or are part of ongoing care related to a patient’s single, serious condition or a complex condition.
CY2024 will add the implementation of payment for the services of marriage and family therapists (MFTs) and mental health counselors (MHCs) when billed by these professionals. Additionally, we are finalizing our proposal to allow addiction counselors or drug and alcohol counselors who meet the applicable requirements to be an MHC to enroll in Medicare as MHCs.
This rule will finalize the proposal to allow the Health Behavior Assessment and Intervention (HBAI) services described by CPT codes 96156, 96158, 96159, 96164, 96165, 96167, and 96168, and any successor codes, to be billed by clinical social workers, MFTs, and MHCs, in addition to clinical psychologists.
SimiTree is Here to Help
These changes can be challenging for hospice agencies to navigate. With the help of SimiTree, agencies can optimize their operations and financial performance. SimiTree offers expert guidance on hospice and home health agency operations, compliance, revenue cycle management, and more. Our experts help agencies understand the proposed changes in hospice payment rates and productivity adjustments and develop strategies to adapt to these changes.
In addition, SimiTree provides customized solutions for hospice and home health agencies, helping them improve their quality of care, increase efficiency, and reduce costs. Read more about our outsourced services or consulting services today.
Additional Resources
See the final rule at: https://public-inspection.federalregister.gov/2023-24455.pdf