

CMS Announces FY2024 Physician Proposed Rule
Centers for Medicare & Medicaid Services (CMS) has announced its FY2024 Physician Proposed Rule. Packed with potential changes, this proposal carries implications for a range of sectors, from Home Health to Behavioral Health, Hospice, and Palliative Care. While the proposed rule may not be extensive, its potential financial and operational impacts are substantial.
In this blog post, we will break down the contents of this rule and analyze how the proposed changes might affect organizations and agencies dealing with Home Health, Behavioral Health, Hospice, and Palliative Care. Although the proposals are not numerous, they have the potential to bring about significant financial and operational consequences. Here is a concise overview of a selection of these proposals.
Hospice
A proposal to allow Mental Health Counselors or Marriage and Family Therapists to serve as members of the Hospice Interdisciplinary Group (§418.56 and §418.114)
FFS proposals that may have implications on Home Health, Behavioral Health and Palliative Care:
CPT codes 96202 (a full 60 minutes of time) and an add-on code 96203 (reported after 75 minutes of total time.
In this proposed rule for CY 2024, we include a proposed definition of ‘‘caregiver’’ for purposes of caregiver training services (CTS), discuss the circumstances under which patients may benefit from care involving caregivers, and propose that CTS may meet the conditions for Medicare payment when treating practitioners identify a need to involve and train caregivers to assist the patient in carrying out a treatment plan. We also propose values for each of the CTS codes.
CMS is proposing a “Caregiver” broadly defined as a family member, friend, or neighbor who provides unpaid assistance to a person with a chronic illness or disabling condition.
CMS further clarifies a caregiver is an individual who is assisting or acting as a proxy for a patient with an illness or condition of short or long-term duration (not necessarily chronic or disabling); involved on an episodic, daily, or occasional basis in managing a patient’s complex health care and assistive technology activities at home; and helping to navigate the patient’s transitions between care settings. For purposes of CTS, we also include a guardian in this definition when warranted.
Proposal to add 2 new G-codes for Community Health Integration (CHI) and including Community Health Workers (CHW). CMS proposed to “create two new G codes describing CHI services performed by certified or trained auxiliary personnel, which may include a CHW, incident to the professional services and under the general supervision of the billing practitioner. We are proposing that CHI services could be furnished monthly, as medically necessary, following an initiating E/M visit (CHI initiating visit)
in which the practitioner identifies the presence of SDOH need(s) that significantly limit the practitioner’s ability to diagnose or treat the problem(s) addressed in the visit.
Also included is a new stand-alone G code for “Administration of a standardized, evidence-based Social Determinants of Health Risk Assessment, 5-15 min, not more often than every 6 months.
Home Health Outpatient - Proposal to Remove the Telehealth Frequency Limitations for Certain Codes
There is a proposal to retain the OTPP and PTPP direct supervision requirement for unenrolled PTs or Ots by clarifying that the Proposed RTM general supervision regulation applies only to the OTA and PTA and does not include the unenrolled OT or PT
TABLE 8: 19 "Always Therapy" Service Codes Nominated for Potential Misvaluation
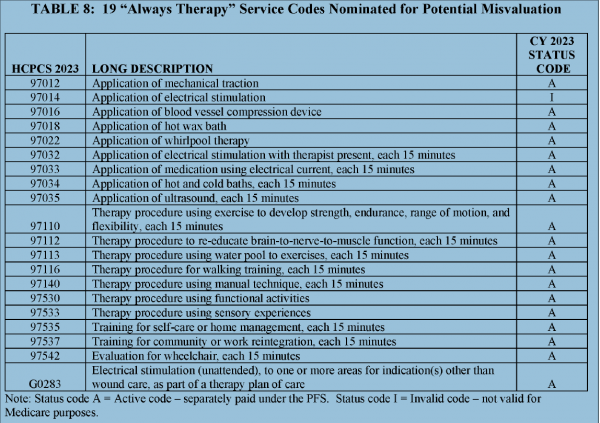
Table 8: 19 "Always Therapy" Service Codes Nominated for Potential Misvaluation
Note: Status code A = Active code - separately paid under the PFS. Status code I = Invalid code - not valid for Medicare purposes.
We have reviewed the clinical labor time entries for these 19 therapy codes, and we are now reconsidering the values established in the CY 2018 final rule. We do not believe that MPPR should be applied to these 19 nominated therapy codes’ clinical labor time entries (listed in Table 8), and as a result, we would like the AMA RUC HCPAC recommendations from January 2017 to be re-reviewed. We recommend the nomination of these 19 codes as potentially misvalued for CY 2024, and we welcome comments on this nomination.
Home Health and Palliative Care
Temporary Addition of Health and Well-being Coaching Services to the Medicare Telehealth Services List
We received a request to permanently add the following three Health and Well-being Coaching services to the Medicare Telehealth Services List:
- CPT code 0591T (Health and wellbeing coaching face-to-face; individual, initial assessment);
- CPT code 0592T (Health and wellbeing coaching face-to-face; individual, follow-up session, at least 30 minutes); and
- CPT code 0593T (Health and wellbeing coaching face-to-face; group (2 or more individuals), at least 30 minutes).
We are not proposing to add these health and well-being coaching services to the Medicare Telehealth Services List on a permanent basis, but we are proposing to add them to the list on a temporary basis for CY 2024. The evidence included in the submitter’s request notes that these codes are similar to others already available on
the Medicare Telehealth Services List. Further, it appears that all elements of these services may be furnished when using two-way interactive communications technology to replace the face-to-face elements of the service.
Changes to CPT code 94762
94762 Pulse Oxymetry recording software (prolonged monitoring 480 min) Equip Code EQ212 is retained, while deleting equipment code EQ353.
95800 – Deleting the equipment codes EQ335 (WatchPAT unit) and EQ336 (oximetry and airflow device) and adding ED021 (computer, desktop, w-monitor (assuming 480 min)
Telehealth Frequency Limitations - CMS Proposes to Remove Frequency Limitation
Proposing to remove the telehealth frequency limitations for the following codes:
- 99231
- 99232
- 99233
- 99307
- 99308
- 99309
- 99310
- G0508
- G0509
We are proposing to remove the frequency limitations for these codes for the duration of CY 2024, which will align with other telehealth-related flexibilities extended by the CAA, in 2023. CMS is broadly assessing our telehealth regulations, in light of the way practice patterns may have changed in the roughly 3 years of the PHE for COVID-19–19 and, while we engage in this assessment, we believe it is reasonable to pause certain pre-pandemic restrictions, such as these frequency limitations, to allow us to gather more information.
SimiTree is Here to Help
To learn more about these proposed changes and how they may impact your organization, fill out our form and we will reach out to you right away. Expert Home Healthcare Consulting Services: Request a Quote » SimiTree (simitreehc.com)